
Early in her pregnancy in 2015, Nicole Hashemi wanted to know how much caffeine was safe for her to consume.
“I was actually advised not to drink a lot of caffeine,” Hashemi, an associate professor of mechanical engineering at Iowa State University, told STAT. The American College of Obstetrics and Gynecologists, for instance, advises that pregnant people consume no more than 200 milligrams per day to reduce the risk of miscarriage or preterm birth.
Hashemi figured there ought to be a way for her to quantify how much caffeine from the tea or coffee she consumed would be transported to her growing baby. Her solution: to build a simplified model of the placenta that would show, using microfluidic technology, just how fluids move through channels and across barriers, in what amounts, and with what effects. She’s one of a handful of biomedical researchers in the U.S. and overseas exploring how the placenta — a notoriously understudied organ, unique in its complexity and impermanence — can be modeled outside the body. The placenta-on-a-chip, as it’s refined in the coming years, could be used to answer research questions and determine the impact of drugs and toxins during pregnancy, these investigators say. “It’s going to be a game-changer for pregnancy studies,” said Ahizechukwu Eke, who leads the maternal-fetal research team and is an associate professor of medicine at Johns Hopkins.
The placenta is a vital organ that plays an important role in the development of a growing fetus. Not only does it form a barrier protecting a fetus from maternal infections and diseases, it also delivers nutrients to and removes waste products from the fetus — even as it constantly changes throughout the duration of pregnancy. For both practical and ethical reasons, it is virtually impossible to study the function of a placenta during pregnancy.
Pregnant people are often excluded from clinical trials to avoid putting the developing fetus at risk and exposing drug companies to legal liability, noted Eke. As a result, physicians rely on studies that don’t have a control group, like pregnancy registries or retrospective cohort studies, to get data. But such databases “are prone to confounding, to misclassifications and to bias,” Eke said. Researchers have also turned to animal testing, pharmacokinetic studies — which simulate the physiological effect of drugs in pregnancy using historical data and models — and sometimes even placental tissue that’s expelled after birth, to study the effects of drugs and other substances. But the results don’t always reliably mirror results from trials with pregnant people.
Last year, Hashemi and her colleagues received a three-year, $350,000 grant from the National Science Foundation to advance their current placenta-on-a-chip model. They plan on designing systems that can be integrated into the model to help collect data in real time. Hashemi told STAT that one system could look at changes in the shapes of cells when exposed to chemicals or physical stressors.
The placenta-on-a-chip technology is simple but potentially powerful, and similar efforts are being made to replicate the environments of other human organs. The small chip is usually about the size of a rubber eraser, etched with tiny channels through which fluids move — offering a simplified, functional model of an organ to test drugs or to study the progression of disease. Researchers can grow cells and run fluids that act like blood through chambers in the chip to create environments similar to those in the human body.
According to Dan Huh, a professor of bioengineering at the University of Pennsylvania and a leader in developing many organs-on-a-chip including the placenta and lung, maintaining the environment is almost like tricking the cells into thinking that they’re still in the body so that they “do what they’re supposed to do.”
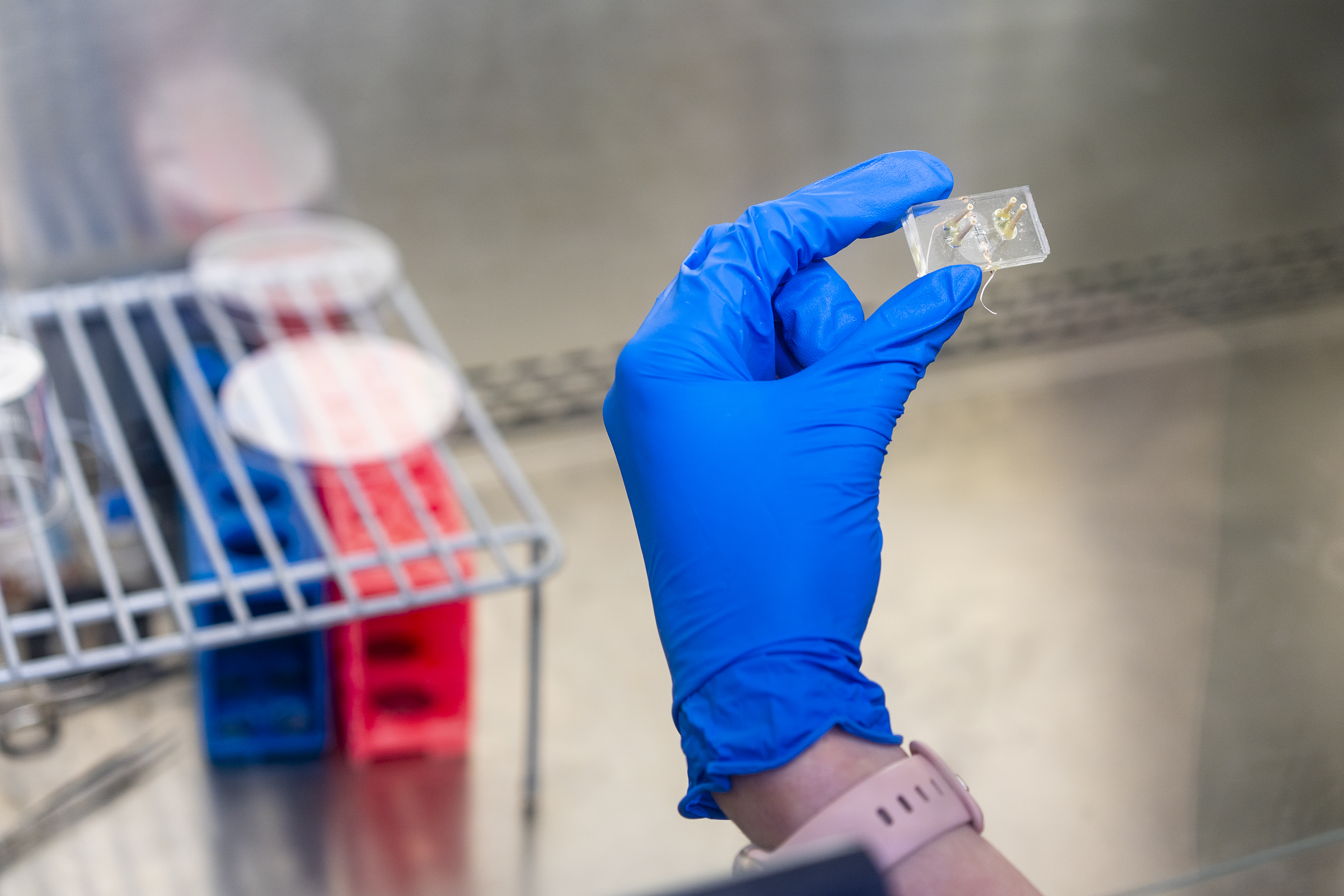
Hashemi’s initial model for a placenta-on-a-chip grew out of her experience working with microfluidic technology to count phytoplankton. Her lab’s chip is a rectangular block made of transparent and flexible silicone with two layers and a porous membrane sandwiched in between them.
Each layer has a microchannel etched into it, which is 100 micrometers in height and 400 micrometers in width. The channels are connected to separate pumps to allow fluid representing blood to flow over the cells. One channel represents maternal blood flow while the other represents fetal blood flow, and the channels are lined with cells that are most commonly found in the placenta. The endothelial cells or the barrier-forming cells protecting the baby are grown on one side of the chamber using human umbilical vein endothelial cells (HUVEC). On the other side are trophoblasts, which provide nutrients to the baby and are grown using an immortalized cancer cell line.
The researchers were able to not only quantify the amount of caffeine that is transported from the maternal side to the fetal side, but they are also able to look at how drugs can affect the fetal side. Besides studying how molecules cross the maternal-fetal blood barrier, Hashemi explained that by running fluids with a higher flow rate, it’s possible to mimic higher blood pressure, which would lead to higher mechanical forces on the cells. In the future, Hashemi hopes to study the effect of mechanical stressors, like preeclampsia, on cells.
“We can predict fairly accurately how nutrients actually get across the placental barrier,” said Huh. Eke agreed, adding that because researchers generally understand the effects of some substances like caffeine on pregnant people, these chips will first validate these established findings and then can be used to answer questions about the effects of unknown drugs.
“So what it tells us that if we use the same model, to study drugs that we don’t have data on in pregnancy, we will be confident to say, ‘OK, we don’t have information on drug x in pregnancy, but based on the placenta-on-a-chip result, we can confidently say that this drug is going to do x, y, z.’”
Huh also mentioned that the model could also look to see how other chemicals, such as environmental toxins like cadmium, can affect the maternal-fetal barrier.
In a 2021 study, Hashemi’s team exposed the maternal channel to naltrexone, which is typically used to treat opioid addiction, but is not recommended in pregnancy due to a lack of data. Hashemi and her colleagues saw that when the endothelial cells or the fetal side were exposed to the metabolized drug, the barrier started to disintegrate after eight hours — in effect validating the recommendation against the use of naltrexone during pregnancy.
So far, the chip’s use is strictly experimental. More data needs to be collected before the chip is submitted to the Food and Drug Administration for approval and can be used by pharma companies as a reliable method to predict what effects a drug will have on a pregnant person. That could take a decade or longer, Eke predicted.
Everything though, is for the patient’s benefit, said Julie Kim, a professor of reproductive science in medicine at Northwestern University, who works with more complicated systems like the reproductive system on a chip. “But there’s a huge gap between what observation you make in a cell culture versus what happens in a woman. And that’s why we want to make systems that are more complicated, yet are able to control.”
Huh and the Wyss Institute started their work on the lung-on-a-chip about 15 years ago, and the field has since expanded to include placenta-on-a-chip, but only a handful of researchers including Huh and Hashemi are working to develop the models further.
In 2022, Huh’s research team published a paper in Nature Communications about a placenta-on-a-chip designed to mimic implantation. He hopes that in the future, this technology could be used to make complicated human body-on-a-chip models to understand the impact of different chemical or environmental exposures and for use in drug development. But creating these integrated systems will be challenging.
It took four years for Hashemi to come up with her model of a placenta-on-a-chip. She didn’t know a lot about the function of placentas when she got started, resources for research were scarce, and at the time, there was no journal dedicated to women’s health that would publish her research. Her caffeine study wasn’t published until 2019.
Now Hashemi is looking to improve on the placenta-on-a-chip model by collecting data in real time — much like digital trackers and glucose monitors do today. “It kind of reminds me of those glucose monitors,” said Kim. “Your body’s still functioning, and it’s able to measure it, and you just wear it and it’s not bothering you. But you’re getting all this data.” Eke said this refinement of the technology to obtain real-time data could eventually allow drugmakers to tailor treatment options and doses.
“Let’s say a baby has a condition that needs to be treated urgently like cancer. You want that drug to be going very fast across the membranes. If a mother has a disease, [clinicians] don’t want that baby to get that disease, so you want that drug to move slowly across the membranes.”
Since she started working on placenta-on-a-chip, Hashemi has been excited to see a younger generation of scientists interested in studying women’s health in general.
But Kim noted that there haven’t been many advances in the development of medicines for women’s health and diseases, especially those that affect the reproductive tract — precisely because studying the biology of the reproductive system, its behavior and its diseases, is difficult, Kim noted. Ex-vivo technologies like placenta-on-a-chip directly address that.
With her initial test of her placenta-on-a-chip model, Hashemi determined that a steady if small amount of caffeine made it over to the “fetal” side after putting in a much greater amount on the “maternal” side. Although she personally wouldn’t tell a pregnant person how much caffeine to drink, Hashemi said she would limit herself to her usual two cups of tea per day.
About the Author Reprints
To submit a correction request, please visit our Contact Us page.












STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect