March 12, 2024

DETROIT — Every morning, Rebecca Smith, nursing a surgically repaired knee, carefully walks down the hallway of her brutalist brick apartment building, takes the elevator one floor to the lobby, and negotiates the sharply angled driveway outside. There, she waits for an Uber to take her to the last place she wants to go: her methadone clinic.
It is her most despised ritual. Smith, 65, is a former medical assistant, a grandmother, and a widow. She has not used illegal drugs in over five years, thanks in large part to methadone, a common medication that is highly effective at treating opioid addiction. But methadone, which once promised Smith freedom from drugs, has made her a prisoner to the drug-treatment system. Like hundreds of thousands of other Americans, she spends each morning journeying to and from her clinic, all so she can wait in line to swallow a small cup’s worth of medication.
Smith’s life has not always revolved around her methadone clinic. Until recently, she was required to show up only once every two weeks. At each visit, she’d take one dose in person, then receive another 13 to take at home. But now, the clinic had forced her to come in each morning: the consequence, it says, for partaking in a celebratory toast at her grandson’s high-school graduation party. Smith, who said she had a few sips from a single glass of wine, was accused by the clinic of “abusing” alcohol and lost the permission to receive her “take-home” doses. No longer free for her early-morning shifts at a catering company, Smith told the clinic doctor that she faced an unthinkable choice. If he wanted her to attend the clinic daily, she’d have to quit her job.
“I’m going to church, I got my bank account, I’m part of society, I’ve got my life in order,” she recalled saying. “It’s been over five years, and you’re gonna do this to me? I said, y’all doing stuff like this makes people go out there and relapse. It’s like you don’t care.”
Smith’s medical records confirm her account. But the clinic was unswayed. As she predicted, Smith was forced to choose her medication over her job. Within weeks, she was late on rent for the apartment she’s lived in for over a decade. In the ensuing three months, Smith dutifully showed up at the clinic each morning. She didn’t consume alcohol or illegal drugs in any quantity. She begged her clinic to restore her take-home doses, restore her freedom, and allow her to return to work. But the clinic hasn’t backed down.
Smith is far from the only patient whose stability, and survival, are being jeopardized by iron-fisted methadone clinics, also known as opioid treatment programs (OTPs). A STAT investigation shows that many of the nation’s methadone clinics rely on controlling and punitive strategies that make it harder, not easier, for patients to maintain their recovery.
There is little evidence to support many of the clinics’ practices. Some clinic staff participating in medical decisions have no training in medicine.


As over 80,000 Americans die each year from opioid overdoses, patient advocates, public health experts, and doctors have increasingly come to question why methadone is accessible only at some 2,000 specialized clinics, many of which enforce outdated rules and offer low-quality care. The immense time commitment that daily clinic visits require, they argue, can also prevent patients from focusing on aspects of life that could aid their recovery, like their work, family, or education.
Though federal regulators recently moved to loosen the regulations governing OTPs, even clinics attempting to provide convenient, compassionate care are still constricted by federal and local policy. Across the country, hundreds of clinics are required to supervise patients while they give urine samples, either in person or through a live video feed; restricted from prescribing doses large enough to alleviate patients’ withdrawal symptoms; and encouraged to taper patients off the medication after a set period, a practice that leading addiction researchers say is dangerous and unsupported by science.
In interviews, leaders in the world of methadone treatment advocacy acknowledged that the system has been slow to evolve since its inception over 50 years ago. But they stressed that the restrictions are intended as a safety measure: Methadone is itself an opioid, and when taken in excess, or in combination with other substances, can cause sedation or even overdose.
“The primary opioid of abuse is fentanyl,” said Mark Parrino, the founder and president of the American Association for the Treatment of Opioid Dependence (AATOD), a national advocacy organization that represents methadone clinics. “When you’re dealing with untreated fentanyl use, the idea of introducing another opiate, methadone, to treat [patients] has risks.”
The strict protocols create a fundamental paradox: People with the most severe addictions are probably the least able to show up at a clinic each morning, and the least able to pay for treatment, which varies widely in price but often costs patients without insurance over $100 per week. As a result, those who need methadone the most are often the people who can access it the least.
Alienated by the clinics’ rigid controls, people who use drugs are often driven away from methadone treatment or never seek it in the first place. At some programs, the high cost of care and lack of flexibility has led many patients to view fentanyl use as a cheaper, easier, and even safer option than enrolling in a methadone clinic.
“By limiting methadone to this one structure, all this power has accumulated in one space,” said Danielle Russell, an advocate, researcher, and methadone patient whose Ph.D. focused on methadone access. “The clinics always make it clear to you that at any moment, they could snatch away a medication that helps you maintain stability and feel safe. There are no other options, and the clinics know that, and they treat you as such. It’s hellacious.”

The most restricted medication
Methadone was developed in pre-World War II Germany as a pain medication, and was first tested as a treatment for opioid addiction in the 1960s. In the U.S., methadone and buprenorphine, another addiction medication, are the only two drugs approved to treat the severe withdrawal and cravings that occur when people who use opioids suddenly stop. In the era of ultra-potent synthetic drugs like fentanyl, patients and doctors alike say it is all but impossible to quit illicit opioids without the aid of either medication.
Methadone is the more effective of the two medications: Research shows that people who take it are 59% less likely to die of an opioid overdose. Despite the magnitude of the U.S. overdose epidemic, however, methadone remains the country’s most difficult medication to obtain. While any licensed doctor can prescribe methadone to treat pain, no doctor is permitted to write a methadone prescription to treat addiction, and patients like Smith can’t simply pick up their medication at a local pharmacy. Instead, they must enroll in specialized clinics that, due to federal law, hold the exclusive right to distribute methadone as an addiction treatment — and therefore hold enormous control over their patients’ lives.
Clinics say these rules are necessary to protect patients. Beyond potential side effects like heavy sweating, weight gain, and sexual dysfunction, methadone can cause overdose when used in excess or in combination with other medications. The risk appears greater when methadone is prescribed to treat pain, not addiction: Washington state, for example, saw a spike in methadone overdoses in the mid-2000s after its Medicaid program and other public insurers, in a bid to save money, began pushing patients toward methadone as an everyday pain drug. As an addiction treatment, too, methadone has risks. One study linked an uptick in methadone-involved deaths from 2019 to 2020 to methadone clinics’ more relaxed practices during the Covid-19 pandemic, though it noted the data “does not allow for a causal attribution.”
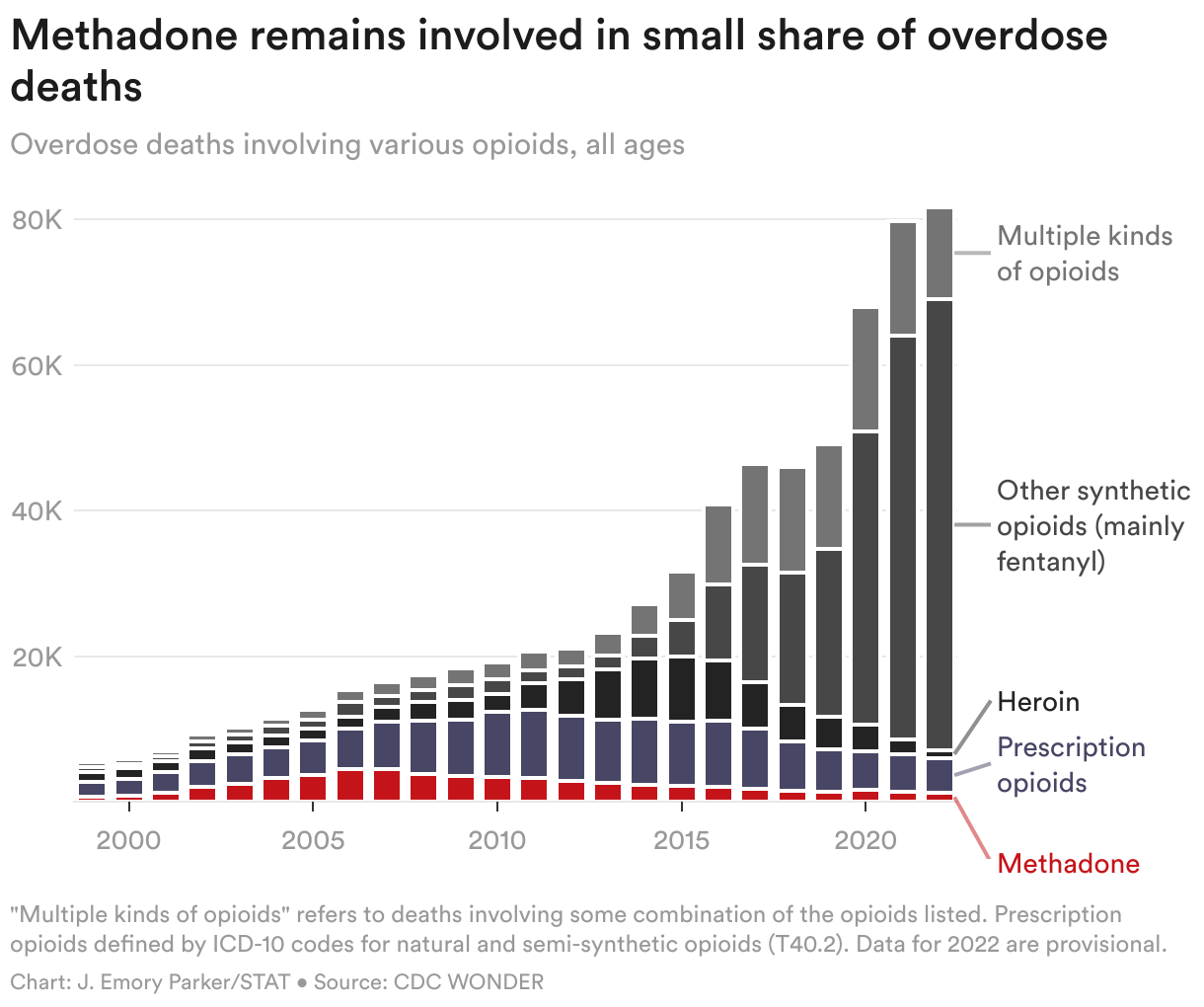
But overall, methadone causes far less harm than other opioids. The annual total of methadone-involved overdose deaths has remained roughly constant over the past decade, even as overall opioid deaths have skyrocketed. Of the 82,807 opioid overdose deaths recorded in 2022, 3,364 involved methadone, according to the Centers for Disease Control and Prevention. Of those deaths, roughly two-thirds also involved an opioid besides methadone, like fentanyl or a prescription painkiller. Research also shows that even as methadone clinics significantly relaxed their restrictions and allowed more take-home medication in 2020, the share of opioid overdose deaths that involved methadone declined.
Still, many Americans view the medication as hardly better than the potent opioids, like fentanyl and heroin, that people taking methadone no longer wish to use. Separately, some clinicians warn that wider access could lead to an increase in overdoses caused by methadone itself.
When patients with severe fentanyl addiction and intertwined mental health conditions seek addiction treatment, high-quality care should entail more than just medication, said Kenneth Stoller, a Johns Hopkins addiction psychiatrist and member of AATOD’s board. To provide methadone without safeguards, he said, could spark even more backlash against a medication that society already views with suspicion.
“All we need are a few front-page stories about how a drug got into the hands of a baby who died of an overdose, or how a person leaving home after taking too much of their medication got into a car accident and killed a family,” he said. “We will see a resurgence of severe stigma toward that medication.”
So far, methadone clinics have gotten their way. Though addiction doctors in Germany, Australia, Canada, and other high-income countries can prescribe methadone directly to patients, in the U.S., it remains available only at specialized opioid treatment programs.

Indignities and red tape
Patients at methadone clinics go to extraordinary lengths to receive their medication, complying with rules and suffering indignities that would be unthinkable in any other health care setting. Patients commonly sign lengthy contracts agreeing to abide by clinic policies, and are often required to participate in frequent drug tests and counseling sessions as a condition of receiving their medication. In interviews, several patients, across multiple clinics, reported that they were admonished by clinic staff for not saying “please” or “thank you.”
Even minor violations of clinic rules can result in major punishments. The total submissiveness that methadone treatment typically requires has led patients to bestow the medication with a damning nickname: “liquid handcuffs.”
Above all, clinics’ rules center on the requirement that patients come in each day to receive their dose. Some are eventually granted “take-home privileges,” in methadone clinic parlance. Others, however, have attended their clinics daily for years without “earning” take-homes.
Often, patients who do receive take-homes must comply with strict rules that clinics say are designed to prevent misuse: They must bring a locked container to the clinic to store their doses, and bring back all of their empty methadone bottles every visit. Patients are also frequently subjected to “call-backs”: being told, without warning, that they have mere hours to show up at the clinic for inspection, medication bottles in hand. Punishment for not showing up for a call-back or a missing bottle may include having take-home doses reduced or rescinded entirely, leaving patients constantly at their clinics’ beck and call.
“Every methadone clinic has got to look very deeply at themselves, and at their current policies, and they need to be rewritten,” said Ruth Potee, an addiction doctor who runs several methadone clinics in Massachusetts. “If you have not changed the number of take-home bottles you’re giving, then shame on you.”
While clinics cast daily in-person dosing as a safety measure, patients and some leading addiction doctors increasingly argue that the requirement is harmful and in many cases unnecessary. For those attempting to move forward from their addiction, clinic visits provide a daily reminder of a history they’d rather forget. Others attempting to stay sober find the visits to be a distraction, or even a threat to their recovery: In interviews, multiple patients reported being offered illicit fentanyl for sale while they waited in line.
Daily dosing also poses logistical hurdles that force patients to structure their lives around their clinics’ dosing hours. Kevin Saunders, who attends a clinic in Biloxi, Miss., recounted a 5:30 a.m. frenzy each day as patients waiting for their clinic to open repeatedly pressed a button on a cellphone app, waiting for an automated system to assign them a place in line. Hitting the button just a few seconds late, he said, could be the difference between waiting five minutes and waiting an hour.
Ryan Fisher of Buckeye, Ariz., said he was denied take-homes despite consistent attendance and negative drug tests because the nearest clinic — located in Phoenix, a nearly two-hour round trip — misplaced his records, accused him of skipping appointments, and made no allowances for absences he had verified were due to his work schedule. Fisher eventually decided methadone treatment wasn’t worth the expense and inconvenience of driving over 400 miles each week. He quit the medication cold turkey, a process he described as “the worst three months of my life.”
Some patients spoke fondly of their counselors, crediting them with providing structure and guidance that helped them remain in treatment and move past their addiction. Others, however, cast the requirement that they participate in counseling as an obstacle to their care, or a means of boosting their clinics’ revenues. Russell, the methadone treatment researcher, said her counseling appointments at a Phoenix-area clinic often consisted solely of making sure she had paid her most recent clinic bills. She has since moved to Australia for a postdoctoral fellowship — and because methadone there is far easier to access.
“Every methadone clinic has got to look very deeply at themselves, and at their current policies, and they need to be rewritten.”
Ruth Potee, addiction doctor
Little data is available about the quality of counseling at methadone clinics, and there is no federal standard for counselors’ qualifications. Longstanding federal guidelines acknowledge that many states “permit non-licensed addictions counselors” who “may be qualified for their positions through training, education, and/or experience.” One federal report from 2019 found “great diversity” and a “lack of a standard model” for counseling services offered alongside methadone or buprenorphine treatment.
Parrino, the head of the clinics’ advocacy group, acknowledged that in some cases, clinics fail to offer high-quality counseling.
“Why do we need counseling if the counseling is crap? It’s a fair question,” Parrino said. “This is where I happen to be aligned with the patient advocacy groups, and always have been: If the program is counter-therapeutic, if the policies are counter-therapeutic, if you’re not engaging patients, if you’re antagonizing or alienating the patients, you have to question what you’re doing.”
Patients also reported alienating experiences related to drug testing. Some clinics require supervision while patients provide a urine sample either via camera or even from inside a bathroom stall. Many clinics use drug tests to determine whether their patients still use illicit substances, and shape their medical decisions accordingly. But clinics also commonly use the tests as justification to restrict take-home medication and to require their patients to attend more frequently — not just when they test positive for illegal drugs or alcohol, but also, in some cases, when patients test positive for marijuana, even in states where marijuana is legal.
Other patients said their clinics made it difficult to receive methadone doses that adequately quelled withdrawal symptoms throughout their 24-hour dosing interval. Beth Miller, who recently switched to a clinic in Connecticut, said her new provider has balked at requests to raise her dose to the level she safely took for 14 years while living a short drive away in Rhode Island.
And while many patients prefer to split their dose in half so that they don’t begin to feel withdrawal symptoms later in the day, many clinics insist that they take it all at once.
On the whole, the patients who recounted their experience said the clinics’ rigid policies made methadone treatment so difficult that some contemplated swearing off the medication altogether. In many cases, those who did returned to using heroin or fentanyl almost immediately.
“Almost every single person I know who has overdosed has been on methadone at some point, and couldn’t hack the restrictions or was terminated for some arbitrary reason,” said Caty Simon, an advocate with the Urban Survivors Union and co-author of the “Methadone Manifesto,” a 2021 call for major reforms to the methadone treatment system.
These practices speak to the same fundamental issue, said Potee, the Massachusetts addiction doctor. Many methadone clinics’ behavior isn’t designed to reduce patients’ odds of overdose, relapse, or death, she argued — instead, it’s geared toward maximizing billable events and minimizing the risk of “diversion,” when clinic-prescribed methadone is misused or sold on the black market.
“Quality of care for patients is driven by the financial bottom line,” she said.
‘From a punitive place’
When the Nixon administration legalized methadone treatment in the 1970s, it viewed the system more as a crime-reduction tool rather than a means of providing health care. Experts on both sides of the methadone debate acknowledge that the system hasn’t fully moved past its “war on drugs” roots: Some clinics still operate largely as they did over 50 years ago.
In an interview, Nick Stavros, the CEO of the fast-growing clinic chain Community Medical Services, acknowledged that the federal regulations that first created the methadone system “came from a punitive place.”
As a country, “we do not treat addiction from a health care perspective,” he said. “We treat it from a punitive perspective. The federal regulations as they previously existed created a power differential where patients had less of a voice in their treatment.”
Parrino, the AATOD president, agreed that the original system created a structure that “would lead to very conservative judgments.” He acknowledged, too, that many workers at OTPs still treat patients more like inmates. But he said those clinics are the exception, and most clinics today display far more compassion for patients than their critics believe.
“I don’t agree with the view that the treatment settings are now more of an incarcerated environment,” he said. “However, in fairness, I would say that there are some program staff that operate as if they were in an incarcerated setting. I do not think it defines the system.”
While some methadone clinics choose to impose cumbersome restrictions on their patients, others do so because they have no choice. At the federal level, and in dozens of states, laws and regulations require clinics to enforce rules that are not based on medical evidence and, in some cases, punish patients in ways that harm their health.
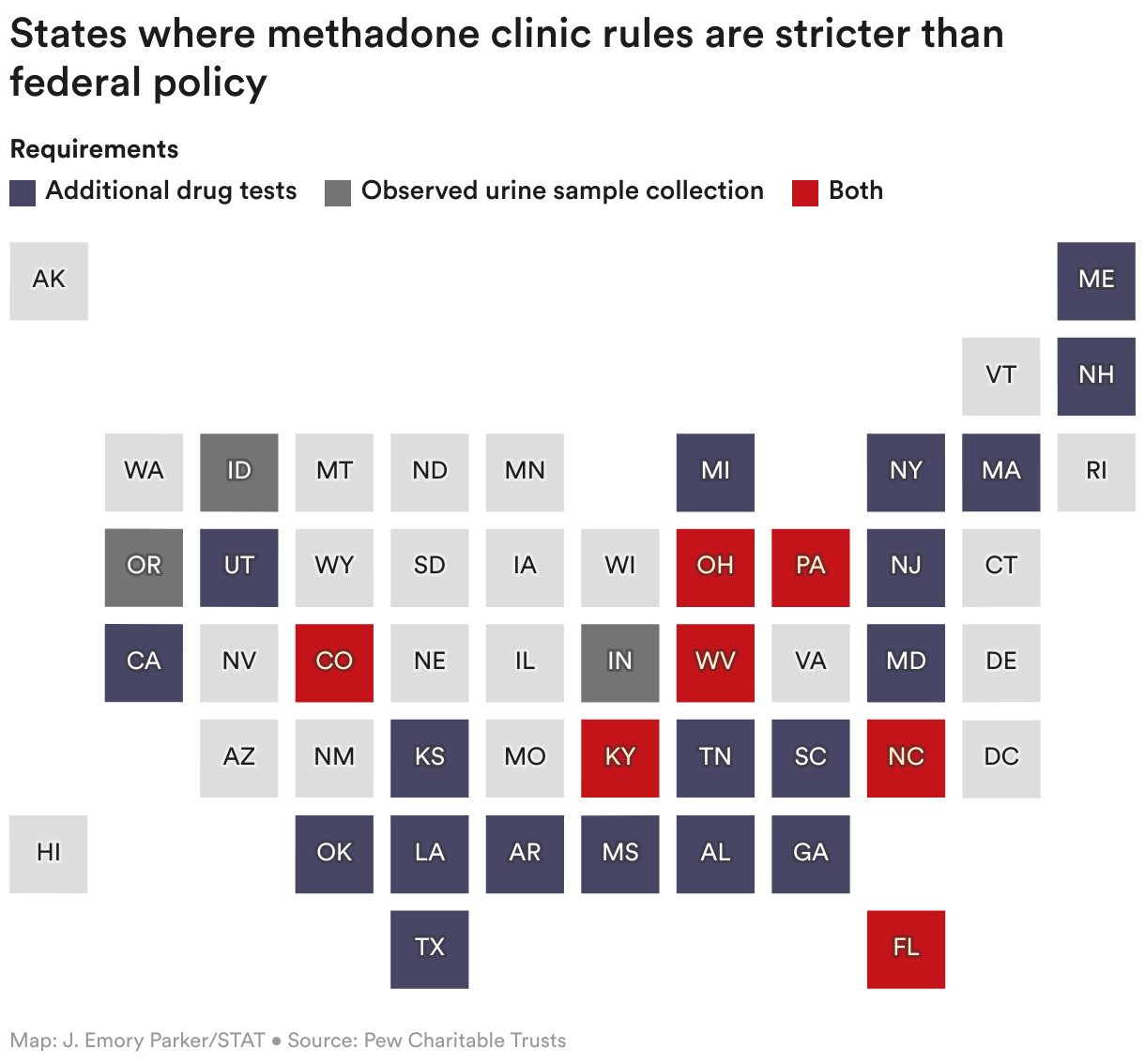
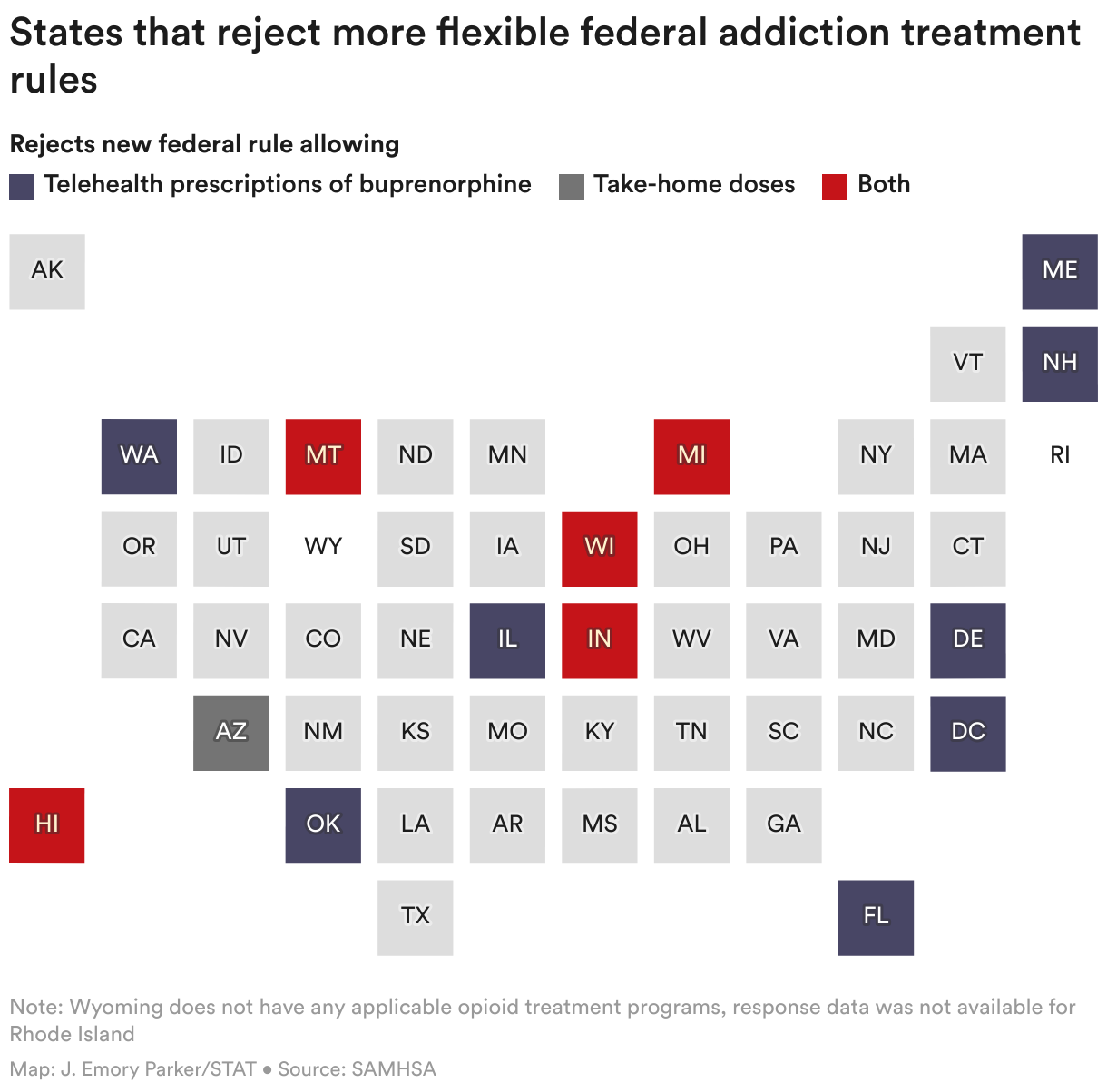
Federal laws require a set number of drug screens and encourage “call-backs” for patients receiving take-home doses. Regulations at the state level can be even more stringent, often mandating a minimum number of counseling sessions as a condition of participating in treatment. Many state regulators, also, have actively opposed the more flexible rules issued by the federal government during the Covid-19 pandemic — namely allowing more generous take-home doses.
According to the Pew Charitable Trusts, eight states also view discontinuation as the ultimate goal of methadone treatment, regardless of medical circumstance, even though the American Society of Addiction Medicine opposes discontinuation absent medical necessity or a patient’s preference. More than 50% of patients return to illicit opioid use within one month of discontinuing medication treatment, according to a recent study.
In every state besides Massachusetts and South Dakota, clinics are allowed to kick patients out for violating program rules. Many addiction experts have stressed, however, that the moments when patients violate program rules — when they use illicit drugs, miss doses, or fail to show up for counseling sessions — are the moments that put them at highest risk for overdose and in the greatest need of treatment. Several states also require clinics to notify regulators before prescribing a methadone dose higher than 120 milligrams, even as some patients attempting to quit fentanyl require doses twice or even three times as high.
In interviews, executives at methadone clinic chains acknowledged that, in many cases, federal and local regulations don’t match their clinical judgment, including requirements that patients participate in a set number of counseling sessions.
“We don’t think people should be forced into it,” said Ben Nordstrom, the chief medical officer of Behavioral Health Group, a major clinic chain. “We operate in some states where there is a minimum counseling frequency, and we have to color within those lines.”
Similarly, Nordstrom said that while he believes marijuana use is clinically irrelevant to his work, state regulations often leave his hands tied.
“I couldn’t care less about smoking pot, and I don’t think anybody I work with cares,” he said. “But if there’s a state regulation that you’ve got to treat cannabis the same way you’d treat cocaine, what do we do?”
Though he welcomed the relaxed federal rules, Nordstrom acknowledged their impact may be limited: The federal government has no power to compel states to treat clinics with more leniency. Likewise, while state regulators can loosen local restrictions, they have no mechanism to compel individual clinics to take advantage of those flexibilities and offer more patient-centered care.
For decades, methadone treatment has also faced intense cultural and political resistance. Last year alone, community activists held protests opposing the opening of new clinics in New York, Washington state, and Virginia. In the 1990s, national figures like Sen. John McCain (R-Ariz.) and former New York Mayor Rudy Giuliani (R) sought to effectively ban funding for clinics. Smith’s birthplace of West Virginia, home to the nation’s highest opioid death rate, has enforced a moratorium on new methadone clinics since 2007.
Despite the cumbersome regulations, some experts say that truly motivated clinic directors could still work within existing rules to provide flexible, compassionate care — and still, many choose not to.
“OTP medical directors have always had the opportunity to be creative and figure out how to provide high-quality care,” said Frances McGaffey, the Pew Charitable Trusts researcher who assembled a comprehensive analysis of state policies governing methadone treatment. “But not all of them have taken advantage of that, or have had the capacity to figure out workarounds.”
‘This is not helping me’
Rebecca Smith was born in January 1959, the ninth of 12 siblings in Hinton, W.Va., a rural town of roughly 5,000 at the time. At 18, she moved to Michigan to be near her uncles — and because, she felt, there were no jobs for Black people in West Virginia.
Her path to heroin, and then to treatment, began nearly three decades ago. By then, Smith had married, settled in Detroit, and started a family. Her husband, Ronald White, worked on the assembly line at Ford Motor Company; she worked as a medical assistant.
But in 1996, White died in his early 40s of pancreatic and liver cancer — a destabilizing loss that led Smith to turn to drugs in an effort to mask her grief.
“It just seemed like I was thrown into the world naked, with nothing,” Smith said. “I love my children deeply. I love them so much. But it was just really hard for me to accept his death. And that’s when I started using.”
The next two decades were a roller coaster: Smith used, then quit, then used more, then quit again. She lost custody of her two youngest children. She was diagnosed with kidney cancer. And she fought her first battle against a methadone treatment provider: After having a kidney surgically removed, Smith said one clinic falsely accused her of drinking too much water in an effort to skew the results of her urine drug screens. The clinic tapered her off the medication without her consent and ejected her from its care. She soon relapsed, kicking off another yearslong cycle of heroin use.
Eventually, Smith settled into the treatment program at Tolan Park Research Clinic in Detroit’s Midtown neighborhood, showing up daily until the clinic finally awarded her multiple days of take-home medication, then a week, then two weeks. She took a job with a catering company owned by her daughter, Tameca.
Smith felt that her redemption arc was complete. She had conquered heroin addiction. She had made amends with her children — including two younger sons who were adopted after child protective services intervened.
Then she celebrated her grandson’s graduation from Cass Tech, a prestigious Detroit high school, with a few sips of wine. The next morning, she went to her clinic to receive her two weeks of take-home doses, meet with her counselor, and “drop” — clinic slang for leaving a urine sample for a drug test.
Alcohol metabolites later showed up on the urine screen, and Smith was honest with her counselor about having partaken in the celebratory toasts.
But staff at her clinic didn’t see the family celebration as a triumph. Though Smith has never exhibited problems related to drinking, Tolan Park accused her of “abusing” alcohol and rescinded her take-home medications.

Smith was forced to quit her job. She does not own a car. Thanks to a recent knee surgery, and an anticipated second procedure she was forced to postpone once the clinic made her attend daily, making the 1-mile journey on foot is not an option. In Detroit, neither is public transportation. Smith, instead, has had to take an Uber each way, every day. Each voyage costs her at least $8, meaning that the clinic rescinding her take-home privileges didn’t just strip her of her income — it also compelled her to spend hundreds of dollars each month on transportation alone.
“I want you to check me if I’m actually doing something wrong and that would hurt me in my recovery,” Smith said. “I’m very serious about my recovery. But this is not helping me in my recovery. This is not doing nothin’ for me, because I don’t feel that I’ve abused anything.”
Smith’s clinic records state her take-home doses were rescinded “due to drinking.” But they make no mention of prior alcohol use, and the doctor’s notes in Smith’s file are nothing but positive: They describe her as “cooperative, calm, pleasant” and her intelligence as “above-average.”
“Patient is here for positive drug screen,” Andrew King, the clinic’s medical director, wrote in a record documenting Smith’s visit. “She had alcohol during a celebration. She freely admits this. She is here to have the discussion about the repercussions of alcohol usage at a methadone clinic.”
The doctor added: “We will be consistent with clinic policy and she will be dosing daily.”
In an email, King declined to comment on Smith’s specific case. But he wrote that addiction care is complicated and requires the balancing of factors including co-occuring mental or physical illness, patient and community safety, and government regulations.
“The treatment of substance use disorders is highly stigmatized and private. It is our policy not to discuss individual patients’ care,” he wrote. “There are many different angles to every story, which are person and context-dependent.”
Pushing for flexibility
As the opioid crisis has grown worse, methadone clinics’ practices have attracted more scrutiny. Lawmakers, patients, and doctor groups like the American Society of Addiction Medicine have called for allowing methadone to be prescribed far more liberally. In a 2019 report, the National Academy of Medicine found that “the current regulations around methadone are not supported by evidence.”
“Many OTP clients simply have no recourse, and nowhere to turn if they are not given take-homes or forced into counseling that doesn’t meet their needs,” said McGaffey, the Pew researcher. “There might be a single OTP within driving distance. Those people just have to comply with rules that don’t fit their lives and don’t make sense for them.”
Clinics are not uniformly rigid or unsympathetic: Increasingly, many offer flexible, patient-centered care that involves higher initial doses and less invasive means of supervised drug testing, like using saliva swabs instead of urine samples. Take-home medication has become far more common, thanks to the pandemic-era rule changes.
The clinics that choose to be more flexible will get a boost from a significant overhaul of federal regulations that take effect next month. Besides making more take-home doses a permanent option, the new rules allow higher initial doses. They also warn clinics against using toxicology testing “punitively” — in effect, warning against treating patients the way Tolan Park has treated Smith.
Many patient advocates say the changes don’t go nearly far enough — and a select few call for abolishing the methadone clinic system entirely.
But Nora Volkow, the director of the National Institute on Drug Abuse, advocated for a middle ground that echoes one popular proposal from Sen. Ed Markey (D-Mass.): allowing the additional option of doctors to prescribe methadone directly to patients, who’d pick the medication up at a pharmacy.
“We need the opioid treatment programs, but it need not be so restrictive,” said Volkow. “There’s no reason we cannot have both: Those that see the value of attending the OTP continue, while at the same time make it easier for patients to be able to get their methadone [from] their physician, or in a pharmacy.”
Even if the clinic monopoly were to be broken, it’s unclear how many non-clinic doctors would be willing to prescribe methadone, especially given the scrutiny that opioid prescribers face in the wake of the prescription opioid oversupply crisis of the early 2000s. Separately, many pharmacies already decline to stock buprenorphine. It stands to reason that many would also refuse to stock methadone.
“This is a good opportunity to completely reexamine how treatment is offered to patients,” said Parrino, the AATOD president. But offering methadone outside the context of an OTP, he said, could easily do more harm than good.
“This is a classic public health risk assessment,” he added. “How many lives will be saved, and how many will die? I don’t know the answer.”

‘She’s not even listening’
Rebecca Smith is still alive.
In the half-year since her clinic radically reshaped her life, she’s never been tempted to return to illicit drugs. She has fully abstained from alcohol — even from champagne toasts at family gatherings. She’s complied with her clinic even as it has forced her to effectively start over as a new patient, “earning” take-home doses in small increments.
Smith relied on her family and her sheer determination to stay healthy. At last, the modest take-home privileges that her clinic recently restored have allowed her to return to work. In another few months, her clinic has indicated it may finally give back the freedom she previously enjoyed: One visit every two weeks, and 13 days of take-home medication in between.
But she knows others aren’t so lucky. Across the country, other patients have been ejected from clinics, had take-home doses rescinded, or been forced to withdraw from treatment programs because of restrictions they couldn’t keep up with.
“They’re making it easier for me to relapse, in a way, because of some of the rules they’re trying to throw at you,” Smith said. “I’m pouring my heart out to my counselor. But it’s like she’s not even listening to me, and the doctor’s not even listening to me. I still feel like a second-class citizen.”
STAT’s coverage of chronic health issues is supported by a grant from Bloomberg Philanthropies. Our financial supporters are not involved in any decisions about our journalism.
About the Author
To submit a correction request, please visit our Contact Us page.






STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect